By Ted Rosen, MD, FAAD, Editor-in-chief
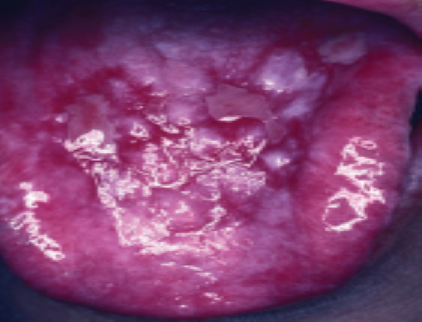
Erosive lichen planus, commonly encountered on the oral mucosa, is notably symptomatic (pain) and often difficult to treat.
Topical ultrapotent and systemic corticosteroids are considered the first-line treatments of choice. However, systemic steroids carry a plethora of potential side effects, and topical steroids may be difficult to utilize effectively in the mouth.
While topical calcineurin inhibitors (TCIs), especially pimecrolimus, are considered the second-line therapy, the burning and stinging accompanying application may dissuade some patients from adherence to any regimen which includes TCIs.
Oral immunosuppressants are certainly convenient and frequently may be effective, but they include significant risks such as gastrointestinal intolerance, infection, and carcinogenesis. Mycophenolate mofetil is probably the safest of these drugs but is notoriously slow in its onset of action.
Therefore, we are still in search of a relatively safe, consistently effective, and convenient manner in which to treat oral erosive lichen planus.1
Recent work on the etiopathogenesis of lichen planus suggests substantial upregulation of the Janus kinase signal transducer and activator of transcription (JAK-STAT) pathway.2 Thus, it is not too surprising that a recent publication chronicled the nearly miraculous resolution of previously recalcitrant severe oral erosive lichen planus following the administration of the selective Janus kinase (JAK) 1 inhibitor, upadacitinib.3
The dose employed was 15 mg daily. This is also consonant with additional case reports of other lichen planus variants responding favorably to JAK inhibitors. I have now used this same modality—upadacitinib–to successfully treat both oral erosive and erosive esophageal lichen planus.
Of course, questions still remain. Which specific category of JAK inhibition will prove to be the most reliable therapy for erosive lichen planus? How durable will the positive effect be? Will any new, unexpected adverse events appear in conjunction with this type of treatment for this type of disease?
Still, I suggest that if you are faced with this really terrible disorder, where those afflicted sometimes can’t even eat or speak comfortably, please remember and consider the JAK inhibitors.
References
- Gupta S, Ghosh S, Gupta S. Interventions for the management of oral lichen planus: a review of the conventional and novel therapies. Oral Dis. 2017;23(8):1029-1042. doi:10.1111/odi.12634.
- Shao S, Tsoi LC, Sarkar MK, et al. IFN-γ enhances cell-mediated cytotoxicity against keratinocytes via JAK2/STAT1 in lichen planus. Sci Transl Med. 2019;11(511):eaav7561. doi:10.1126/scitranslmed.aav7561.
- Balestri R, Bortolotti R, Rech G, et al. Treatment of Oral Erosive Lichen Planus With Upadacitinib. JAMA Dermatol. 2022;158(4):457-458. doi:10.1001/jamadermatol.2022.0147
